Introduction
Menopause, the permanent cessation of menstruation, is a universal physiological transition that women experience, typically occurring between the ages of 45 and 55 [1]. It is estimated that over 500 million women worldwide are currently experiencing menopause, with projections indicating a significant increase in this number as the global population ages [2]. While menopause is a natural biological process, it is often accompanied by a constellation of distressing symptoms, collectively referred to as menopausal syndrome [3]. These symptoms vary widely in type and severity, ranging from vasomotor symptoms like hot flashes and night sweats to psychological manifestations such as mood swings, anxiety and depression, as well as urogenital problems like vaginal dryness and decreased libido [4].
The impact of menopausal symptoms on women’s quality of life is substantial. Vasomotor symptoms, in particular, lead to disrupt sleep, impair concentration and negatively affect work productivity [5]. Psychological symptoms can exacerbate existing mood disorders or trigger new ones, leading to social isolation and decreased life satisfaction [6]. Additionally, urogenital symptoms can significantly impact sexual function and overall well-being [7]. The cumulative effect of these symptoms poses a significant burden on women’s physical and mental health, with implications for their overall quality of life and productivity.
Conventional and alternative approach for menopausal symptom management
To manage menopausal symptoms, women often seek various treatment options. Hormone replacement therapy (HRT) has been a conventional treatment for decades, providing relief for many women. However, concerns have been raised about the long-term safety of HRT, including increased risks of breast cancer, stroke and cardiovascular disease [8]. These concerns, in parallel with individual preferences and cultural considerations, have surged the search for alternative and complementary therapies.
In this context, Ayurveda and Siddha, which are traditional Indian systems of medicine with a holistic approach to health and well-being, have emerged as a potential avenue for menopausal symptom management [9]. Rooted in rich history spanning thousands of years, both Ayurveda and Siddha offer a comprehensive framework for understanding and addressing health concerns, emphasizing the interconnectedness of mind, body and spirit. Ayurvedic and Siddha principles and practices encompass a wide array of modalities, including herbal therapies, dietary recommendations, lifestyle modifications and individualized treatment plans tailored to each person’s unique constitution [10].
Ayurveda and Siddha: similarity and difference
Ayurveda and Siddha, indigenous Indian medical systems, share a common philosophical foundation rooted in holistic health principles that emphasize the interconnectedness of mind, body and spirit. Both systems recognize the vital role of maintaining equilibrium among the fundamental bodily energies, known as doshas (Vata, Pitta and Kapha) in Ayurveda and Mukkuttram in Siddha, which govern physiological and psychological functions. Imbalances in these energies are considered the underlying cause of disease, and restoring balance through various therapeutic modalities is central to both systems [9,11].
Herbal medicine is a cornerstone of both Ayurvedic and Siddha practices, with each utilizing a diverse array of medicinal plants, minerals and metals for therapeutic purposes. However, the specific herbs employed, their combinations and preparation methods often differ. Ayurveda typically favors herbs with broad therapeutic actions, while Siddha may utilize herbs with more potent and targeted effects [12]. Lifestyle modifications, encompassing dietary adjustments, exercise regimens and stress management techniques, are integral to both systems. Both emphasize the importance of a balanced diet, regular physical activity and adequate rest for maintaining health and preventing disease [13]. However, specific recommendations tend to vary based on individual constitutions and health conditions.
Personalized treatment plans are another hallmark of both Ayurveda and Siddha. Both systems recognize individual variability in constitution (Prakriti in Ayurveda, Udalkattu in Siddha), which influences disease susceptibility and treatment response [14]. Therefore, individualized assessments and tailored treatment plans are crucial in both systems, considering the unique physical, mental and emotional characteristics of each individual. Despite their shared principles, Ayurveda and Siddha exhibit notable differences. Ayurveda is more widely practiced across India and boasts a more extensive body of classical literature, while Siddha is predominantly practiced in southern India, particularly Tamil Nadu [14,15]. Furthermore, Ayurveda is often perceived as more theoretical and philosophical in its approach, whereas Siddha emphasizes observation and experiential knowledge in the healing process [13].
Potential of Ayurvedic and Siddha for menopausal symptom relief
Preliminary evidence from both traditional knowledge and modern research suggests that Ayurvedic and Siddha interventions hold promise for alleviating menopausal symptoms. Numerous Indian herbs, such as Ashwagandha, Shatavari and Ashokarishta, have been traditionally used to support women’s health and possess properties that address hormonal imbalances, mood fluctuations and other menopausal complaints [16]. Additionally, Ayurvedic and Siddha lifestyle practices, including yoga, meditation and specific dietary recommendations, contribute to overall well-being and symptom reduction.
While the existing evidence base for Ayurvedic and Siddha interventions in menopause is still evolving, a growing number of clinical trials are exploring their efficacy and safety. These trials have investigated a variety of herbs, formulations and lifestyle modifications, with promising results in reducing hot flashes, improving mood, enhancing sleep quality and addressing other menopausal symptoms. However, the methodological quality and heterogeneity of these studies necessitate a systematic and rigorous evaluation of the available evidence.
Aim of the work
The current systematic review aims to assess the existing clinical trial evidence regarding the efficacy and safety of Ayurvedic and Siddha interventions for managing menopausal symptoms in women. The review will specifically address the following research questions:
– What is the current evidence regarding the effectiveness of herbal therapies and formulations in reducing menopausal symptoms compared to placebo or conventional treatments?
– What are the potential adverse effects and safety concerns associated with Ayurvedic and Siddha interventions for menopausal symptom management?
– What are the optimal dosages and durations of Ayurvedic and Siddha therapies for managing menopausal symptoms, and do they vary depending on individual characteristics or symptom profiles?
Methods
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17].
Search strategy
A comprehensive search strategy was implemented to identify relevant studies. The following electronic databases were searched from 2010 to March 2024: PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL) and Ayurveda-specific databases like the Digital Helpline for Ayurveda Research Articles (DHARA) and the Central Council for Research in Ayurvedic Sciences (CCRAS) database. The search terms included a combination of MeSH terms and free-text terms related to menopause, Ayurvedic/Siddha medicine and herbal interventions. The search strategy was adapted for each database, and no language restrictions were applied. Additionally, the reference lists of included studies and relevant review articles were manually searched for potential studies.
Eligibility criteria
Studies were included if they met the following criteria: (1) randomized controlled trials (RCTs) or quasi-RCTs; (2) included women diagnosed with menopause or perimenopause; (3) evaluated Indian Traditional Medicine interventions (Ayurveda/Siddha), including herbal therapies, formulations or lifestyle modifications; (4) reported outcomes related to menopausal symptoms, quality of life or hormonal parameters; and (5) were published in English. Studies were excluded if they were non-randomized, did not specifically address menopausal symptoms or were published in languages other than English.
Data extraction
The study investigators extracted data from the included studies using a standardized data extraction form. The extracted data included study characteristics (e.g. author, year, location, study design, sample size), participant characteristics (e.g. age, menopausal status), details of the Ayurvedic and Siddha intervention (e.g. herb/formulation, dosage, duration) and outcome measures (e.g. menopausal symptom scores, quality of life, hormonal levels).
Study selection
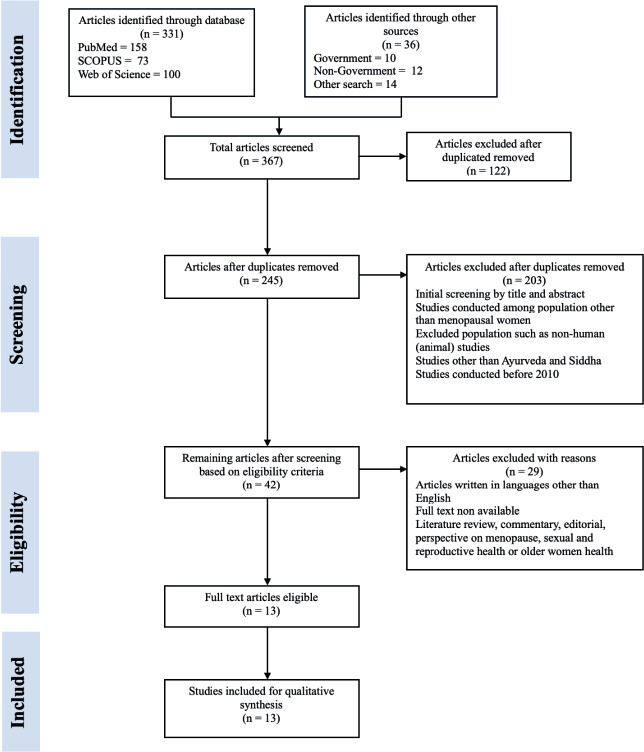
The initial literature search yielded 367 articles from various databases and sources. After removing duplicates, 245 articles remained for title and abstract screening. Of these, 232 articles were excluded due to not meeting the inclusion criteria, primarily because they were not RCTs or did not investigate Ayurvedic or Siddha interventions for menopausal symptom management. The remaining 13 studies met all the eligibility criteria and were included in the final qualitative synthesis. Of the 13 studies included, 7 were Ayurvedic trials, 3 were Siddha trials, and 4 involved a combination of both systems. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
Risk of bias assessment
The risk of bias in the included studies was assessed by the authors using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized trials [18]. The RoB 2 tool evaluates five domains of bias: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome and bias in selection of the reported result. Each domain was rated as “low risk”, “some concerns” or “high risk” of bias.
Data synthesis and analysis
Due to the heterogeneity of the interventions, outcome measures and study designs, a meta-analysis was not deemed appropriate. Therefore, a narrative synthesis was conducted to summarize the findings of the included studies. The results were organized and presented according to the type of Ayurvedic/ Siddha intervention (e.g. herbal therapy), specific herb or formulation used and the primary and secondary outcomes reported. A summary of findings was created to present the main findings of the included studies. Additionally, a qualitative synthesis was conducted to identify common themes and patterns across the studies, highlighting the potential benefits and possible risks of Ayurvedic/Siddha interventions for menopausal symptom management.
Literature review results
Data analysis
In this systematic review, 13 studies met the inclusion criteria and were assessed for their methodological quality and efficacy in utilizing Ayurvedic/Siddha interventions for menopausal symptom management. The following sections emerged as themes describing the characters and efficacy of the intervention tested. A summary of the included studies, along with their key characteristics and outcomes, is presented in Table 1. The dosages, duration, efficacy and adversity of the interventions are summarized in Table 2. In addition, Table 3 describes the key herbal therapies used as intervention in the RCT with its scientific terminology and brief description.
Table 1
Characteristics of the studies including country of origin, population, age group, sample size, intervention (herbal therapies/panchakarma) and outcome (chronological order)
| Authors (Year) | Country | Population | Age group | Sample size | Intervention | Outcome | Approach | |
|---|---|---|---|---|---|---|---|---|
| Herbal therapies | Panchakarma | |||||||
| Santwani et al., 2010 [19] | India | Women not having menses for at least6 months | 40-55 | 43 | Saraswatarishta | Shirodhara | Significant relief in psychic and somatic symptoms with Shirodhara and Saraswatarishta comparedto HRT. | Ayurvedic |
| Modi et al., 2012[16] | India | Menopausal women without surgical menopause | 40-55 | 51 | Ashokarishta, Ashwagandha Churna and Praval Pishti | None | 78.43% of patients experienced mild improvement, and 17.65% had moderate improvement, with no patients completely cured.Serum calcium levels increased by 2.62%,indicating a positive effect on calcium metabolism | Ayurvedic and Siddha |
| Shamshad Begum et al., 2016[24] | India | Menopausalwomen | 45-58 | 88 | Fenugreek (Trigonella foenum-graecum) called FenuSMART™ | None | Significant improvement in the quality of life of participants in the fenugreek extract(FenuSMART™) group, showing reduced physical and mental fatigue, enhanced interest in daily activities, stability of mind, and concentrationcompared to the placebo group. | Ayurvedic |
| Fatima and Sultana, 2017[30] | India | Menopausalwomen | 40-55 | 60 | Gokshura(Tribulus terrestris) | None | Tribulus group showed a 63.4% reduction in joint and muscular discomfort, outperforming the placebo group’s 37.8% reduction.Substantial decrease in depression and moodchanges. | Siddha |
| Huber et al., 2017[26] | Germany | Menopausalwomen | 45-55 | 78 | Pomegranate seedoil | None | Symptom improvements were particularly notable in vasomotor symptoms, psychological symptoms, and urogenital symptoms.PSO treatment did not significantly affect17ß-estradiol levels. | Ayurvedic |
| Steels et al., 2017[25] | Australia | Menopausalwomen | 40-65 | 104 | T. foenum-graecumde-husked seed extract (Libifem®) (Fenugreek) | None | Significant improvement in being impatient with others and feelings of wanting to be alone compared to the placebo groupImprovement in memory, anxiety and depressionin the active treatment group. | Ayurvedic |
| Tomar et al., 2017[28] | India | Menopausalwomen | 40-55 | 116 | Ashokarishta, Ashvagandha Churna and PravalaPishti | None | Increase in quality of life and reduction in adversity of menopausal symptoms.74.17% reduction in psychological symptoms at 12weeks and 75.87% at 14 weeks. | Both Ayurvedic and Siddha |
| Steels et al., 2018[20] | Australia | Healthy women | 40-65 | 117 | Tinospora cardifolia, Asparagus racemosus, Withania somnifera and Commiphora mukul | None | Tinospora cardifolia, Asparagus racemosus, Withania somnifera and Commiphora mukul to be a safe and effective treatment for reducing menopausal symptoms in healthy menopausalwomen. | Ayurvedic |
| Devi et al., 2020[29] | India | Menopausalwomen | 40-55 | 49 | Sukumara Ghritam and Brahmi Churnam | None | Significant improvements in somatic, psychological, and urogenital symptoms were observed, with reductions of approximately68.3%, 80.1%, and 63.7%, respectively. | Siddha |
| Khanna et al., 2020[23] | India | Menopausalwomen | 39-51 | 48 | Proprietary hydro-ethanolic extract of fenugreek seeds (Trigonella foenum-graecum) | None | Significant improvement in somatic, psychological, and urogenital symptoms in perimenopausal participants.Increase in total and free testosterone levels in the FHE group, correlated with a decrease in sexhormone binding globulin (SHBG) levels. | Ayurvedic |
| Gopal et al., 2021[22] | India | Menopausalwomen | 40-55 | 100 | Ashwagandha (Withania somnifera) | None | Ashwagandha root extract significantly improved vasomotor, psychological, and somato-vegetative symptoms compared to the placebo group. It also led to a reduction in serum estradiol levels and an increase in serum FSH and LH levels, indicatinga positive impact on hormonal balance. | Both Ayurvedic and Siddha |
| Sakhare and Rajendra, 2021[27] | India | Perimenopausal women | 40-55 | 32 | S-GABA Churn (An indigenous formulation, consistingShatavari, Guduchi, Ashwagandha,Brahmi, Amalaki) | Nasya Karma with Kalyanaka Ghrita | Combined intervention of Kalyanaka Ghrita Nasya Karma and S-GABA Churna led to statistically highly significant improvements in psychological, somatic and vasomotor symptoms of perimenopausal syndrome. | Both Ayurvedic and Siddha |
| Gudise et al., 2024[21] | India | Premenopausal and postmenopausalwomen | 40-65 | 70 | Shatavari (Asparagus racemosus willd)Aspurūs™ | None | Significant decrease in psychological symptoms, as well as somatic symptoms like fatigue and pain. The reduction in symptoms was statisticallysignificant within and between treatment groups. | Siddha |
Table 2
Dosages, duration, efficacy (psychological and somatic), standardized scales and adverse health effect of the interventions
| Authors (Year) | Dosage | Duration | Efficacy | Menopausal rating scales | Adverse health effect | |
|---|---|---|---|---|---|---|
| Psychological symptom reduction | Somatic symptom reduction | |||||
| Santwani et al., 2010[19] | Group A received conjugated estrogens 0.625 mg once daily for 45 days.Group B received saraswatarishta 20 ml mixed with water and taken before meals twice a day for a duration of 45 days.Group C received shirodhara with Bala Taila for 30 minutes per sitting. | 45 Days | Moha (delusion, Krodha (anger), Shoka (grief), Bhaya (fear), Medha (intellect), Smriti (memory, anxiety, depression, irritability tension, suicidal tendencies) | Headaches, joint pains, backache, constipation, dyspepsia, palpitations, decreased libido, muscular aches, tingling sensations, hot flushes, frequent urination, flatulence, sleep problems | Manasa ParikshaBhavas,Hamilton’s Anxiety Rating Scale Menopause Rating Scale | None |
| Modi et al., 2012 [16] | 25 ml Ashokarishta twice daily with an equal quantity of water after food3 g Ashwagandha Churan and 1 capsule of 250 mg Praval Pishti twice daily with milk 1/2 hours before food | 3 months with one week follow-up | Depressive mood, irritability, anxiety and physical and mental exhaustion | Hot flushes, heat discomfort, sleep problem, sexual problems, bladder problem, dryness of the vagina and joint/muscular discomfort | Menopause-Specific Quality of Life (MENQOL) questionnaireMenopause RatingScale | No adverse health effect reported |
| Shamshad Begum et al., 2016[24] | Two capsules of 250 mg each per day for the first week, followed by an increase to four capsules per day (250 mg each) forthe subsequent 12 weeks | 90 days | Depression and anxiety | Hot flashes, vaginal dryness, irritability, night sweats, mood swings,insomnia, and headaches | Greene Climacteric Scale (GCS)Short Form-36 (SF-36®) Health Survey | None |
| Tomar et al., 2017[28] | 25 ml Ashokarishta twice daily with an equal quantity of water after food3 g Ashwagandha Churan and 1 capsule of 250 gm Praval Pishti twice daily with milk 1/2 hours before food | 3 months with two weeks of follow-up | Mood Swings, irritability, anxiety and emotional disturbance | Joint pain, muscle aches and headaches | Menopause-Specific Quality of Life (MENQOL) questionnaireMenopause RatingScale | None |
| Fatima and Sultana, 2017[30] | 3 g powder of Tribulus or placebo twice daily | 8 weeks | Depressive moods | Joint pain, muscle aches and headaches | Menopause Rating Scale (MRS) | None |
| Huber et al., 2017[26] | 1000 mg of PSO daily in 2 capsules | 8 weeks | Depression, irritability, and anxiousness | Vasomotor symptoms (e.g., hot flushes), physical and mental exhaustion, and sleeping problems | Menopausal Rating Scale (MRS)17ß-Estradiol Levels Subjective Efficacy and Tolerability Ratings | Gastrointestinal issues suchas heartburn, changes in stool consistency, abdominal cramps, and stomach discomfort; additional side effects reported by participants included weight gain, unpleasant taste of the medication,skin problems, and a reset ofmenstruation. |
| Steels et al., 2017[25] | 600 mg per day (1 × 300 mg capsule b.i.d.) with food, at breakfast and with evening meals | 12 weeks | Dissatisfaction with personal life, accomplishing fewer tasks, being impatient with others, feelingsof wanting to be alone | Aching joints, feeling worn out, physical strength, stamina, energy | Menopause-Specific Quality of Life (MENQOL) questionnaire | None |
| Steels et al., 2018[20] | 75 mg Tinospora ardifolia, 100 mg Asparagus racemosus,100 mg Withania somnifera and 225 mg Commiphora mukul | One capsule twice per day overa period of12 weeks | Increased in quality of life accomplishing less tasksdepressionincreased patience | Hot flushes, daytime hot flushes and night sweats body ache, stamina, facial hair, vaginal dryness and avoidance of intimacy | Menopause-Specific Quality of Life (MENQOL) questionnaire | None |
| Devi et al., 2020 [29] | Sukumara Ghritam was administered in a dose of 6 g twice a day with warm water1 hour before food.Brahmi Churnam was administered 3 g orally twice a day with lukewarm water after food. | 84 days with28 days follow-ups | Mood swings, irritability, anxiety, and depression | Physical discomfort and bodily sensations | Menopause Rating Scale (MRS) | None |
| Khanna et al., 2020[23] | 250 mg FHE twice a day, after breakfast and dinner | 42 days | Depressive moods | Hot flushes and night sweats | Menopause Rating Scale (MRS) | None |
| Gopal et al., 2021[22] | 300 mg capsule of Ashwagandha root extract (KSM-66) twice a day | 8 weeks | Depression, irritability, and anxiety | Exhaustion, physical discomfort, and other somato-vegetative symptoms | Menopause Rating Scale (MRS) and the Menopause-Specific Quality of Life (MENQoL)questionnaire | Mild adverse events were reported by participants, including abdominal discomfort, abdominal pain, nausea, andinsomnia. |
| Sakhare and Rajendra, 2021[27] | Nasya Karma with Kalyanaka Ghrita for 7 consecutive days of intervention (2 ml in each nostril in the morning)12gms S-GABA Churna were divided equally in 2 doses after food with warm milk. | 60 days | Reduction in heart beating quickly or strongly, feeling tense or nervous, difficulty in sleep, excitable, attacks of anxiety, difficulty in concentrating, feeling tired or lacking in energy, loss of interestin most things, feeling unhappy or depressed, cryingspells, and irritability | Headache, muscle pain, and hot flushes | Menopause Rating Scale (MRS) | None |
| Gudise et al., 2024[21] | 250 mg capsules containing Asparagus racemosus root extract | Twice a day for 60 days(eight weeks) | Depression, anxiety and stress | Reduction in hot flashes, night sweats, insomnia, anxiety, nervousness, vaginal dryness, and loss of libido | Utian Quality of Life (UQoL) Scale Depression, Anxiety, and Stress Scale RegensburgInsomnia Scale (RIS) | 5 participants experienced six adverse events, including dizziness and bloating. |
Table 3
Key Ayurvedic/Siddha terminology and definitin used in the RCT studies
Efficacy of Ayurvedic and Siddha herbal therapies
The therapeutic potential of herbal therapies in managing menopausal symptoms has been extensively investigated. Several studies have demonstrated their efficacy in alleviating both physical and psychological symptoms. For instance, Santwani et al. [19] showed that Saraswatarishta, an Ayurvedic formulation, significantly reduced both somatic and psychological symptoms compared to HRT, suggesting its potential as an alternative or complementary treatment.
Further studies have explored the effects of specific herbs and combinations. Steels et al. [20] demonstrated the efficacy of a multi-herb formulation containing Tinospora cardifolia, Asparagus racemosus (Shatavari), Withania somnifera (Ashwagandha) and Commiphora mukul (Guggul) in improving vasomotor symptoms, musculoskeletal discomfort and psychological well-being. Gudise et al. [21] found that Shatavari alone significantly reduced both psychological (anxiety, depression) and somatic symptoms (hot flashes, insomnia) in pre- and postmenopausal women. Additionally, Gopal et al. [22] reported significant improvements in vasomotor, psychological and somatic symptoms, as well as hormonal balance, in perimenopausal women treated with Ashwagandha root extract.
Psychological benefits of Ayurvedic herbs
Beyond their effects on physical symptoms, Ayurvedic herbal therapies have also shown promise in managing the psychological aspects of menopause. Santwani et al. [19] noted significant reductions in anxiety, depression and irritability with Saraswatarishta and Shirodhara, while Steels et al. [20] reported improvements in depressive symptoms and overall quality of life with their multi-herb formulation. Shatavari has also demonstrated efficacy in reducing psychological distress, including anxiety, depression and stress, as shown by Gudise et al. [16] Moreover, both Ashwagandha [21], a novel fenugreek seed extract [10, 23-26], and Kalyanaka Ghrita and S-GABA Churna [27] have been shown to significantly improve mood and emotional stability in perimenopausal and menopausal women, respectively.
Somatic symptoms reduction
Ayurvedic herbal therapies have demonstrated promising results in alleviating various somatic symptoms associated with menopause. Steels et al. [20] reported significant reductions in hot flashes, night sweats and vaginal dryness in menopausal women treated with a combination of Tinospora cardifolia, Asparagus racemosus (Shatavari), Withania somnifera (Ashwagandha) and Commiphora mukul (Guggul), underscoring the benefits of these herbs. In a similar vein, Gudise et al. [21] found that Shatavari alone significantly reduced hot flashes, night sweats and insomnia, as measured by the Utian Quality of Life (UQoL) Scale and the Regensburg Insomnia Scale (RIS). Additionally, this study highlighted improvements in overall somatic health, emphasizing the broad-ranging benefits of this herb.
Tomar et al. [28] observed significant reductions in joint pain, muscle aches and headaches in menopausal women treated with a combination of Ashokarishta, Ashwagandha churna and Pravala pishti. This suggests a potential synergistic effect of these combined herbs in addressing various somatic discomforts. Gopal et al. [22] further demonstrated the efficacy of Ashwagandha root extract in reducing physical discomfort, exhaustion and sleep disturbances in perimenopausal women.
Moreover, specific herbs have shown targeted effects on particular somatic symptoms. Devi et al. [29] found that Sukumara Ghritam and Brahmi Churnam significantly reduced physical discomfort and bodily sensations, while Khanna et al. [23] reported significant improvements in vasomotor symptoms (hot flashes and night sweats) with a novel fenugreek seed extract. Additionally, Fatima and Sultana [30] demonstrated a 63.4% reduction in joint and muscular pain with Gokshura (Tribulus terrestris) compared to a 37.8% reduction in the placebo group.
Menopausal rating scales and quality of life
The use of validated rating scales is essential for objectively evaluating the impact of herbal therapies on menopausal symptoms and quality of life. The Menopause-Specific Quality of Life (MENQOL) questionnaire, encompassing vasomotor, psychosocial, physical and sexual domains, provides a comprehensive assessment of the menopausal experience. Steels et al. [20] demonstrated significant improvements across all MENQOL domains with their multi-herb formulation, while Tomar et al. [28] observed enhanced quality of life and reduced symptom severity using both the MENQOL and Menopause Rating Scale (MRS).
The MRS, which assesses somatic, psychological and urogenital symptoms, is another effective tool for quantifying symptom severity. Tomar et al. [28], Gopal et al. [22], Khanna et al. [23], Fatima and Sultana [30] and Devi et al. [29] all utilized the MRS to demonstrate significant reductions in various menopausal symptoms following treatment with different Ayurvedic interventions.
Furthermore, the Utian Quality of Life (UQoL) Scale, designed specifically for peri- and postmenopausal women, offers a unique perspective on the impact of herbal therapies on overall well-being. Gudise et al. [21] employed the UQoL Scale to highlight improvements in sleep quality and other somatic symptoms with Shatavari.
Safety and adverse health effect
Safety assessments of Ayurvedic herbal therapies in the context of menopause management have generally yielded positive results. Steels et al. [20] reported that the combination of Tinospora cardifolia, Asparagus racemosus, Withania somnifera and Commiphora mukul was well-tolerated, with only mild and transient adverse effects such as gastrointestinal discomfort and headaches. Similarly, Gudise et al. [21] found that Shatavari (Asparagus racemosus) was associated with minimal adverse effects, primarily mild gastrointestinal upset, which did not lead to discontinuation of therapy.
Tomar et al. [28] and Gopal et al. [22] also reported favorable safety profiles for their respective Ayurvedic interventions (Ashokarishta, Ashwagandha Churna, Pravala Pishti and Ashwagandha root extract), with most side effects being mild and self-limiting. However, Khanna et al. [23] observed some instances of moderate adverse effects, such as nausea and skin rashes, with a novel fenugreek seed extract, highlighting the need for careful monitoring and individualized assessment.
Fatima and Sultana [30] assessed the safety of various Ayurvedic formulations and found them generally well-tolerated, although occasional allergic reactions were reported. Devi et al. [29] investigated Sukumara Ghritam and Brahmi Churnam, noting only minor side effects like mild gastrointestinal disturbances. In addition, Huber et al. [26], using pomegranate see oil, reported minor adversity including gastrointestinal issues and skin problem. While the overall safety profile of Ayurvedic herbal therapies appears promising, these studies emphasize the importance of individualized patient care thorough assessment and vigilant monitoring for potential adverse effects.
Hormonal balance and biochemical markers
The potential of Ayurvedic herbal therapies to modulate hormonal levels and influence biochemical markers associated with menopause has been a key focus of research. Steels et al. [20] demonstrated that their multi-herb formulation led to significant reductions in follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels, accompanied by increased estrogen levels, indicating improved hormonal equilibrium. Gudise et al. [21] further explored the hormonal effects of Shatavari, finding notable increases in estrogen and decreases in FSH and LH levels, which correlated with reductions in hot flashes and night sweats. Similarly, Tomar et al. [28] reported significant hormonal changes, including increased estrogen and decreased FSH and LH, with their combination therapy, associated with improvements in mood, irritability and quality of life.
Gopal et al. [22] also observed positive hormonal modulation with Ashwagandha root extract, including increased estrogen and decreased FSH and LH levels, contributing to reduced menopausal symptoms. Khanna et al. [23] found that fenugreek seed extract not only influenced estrogen, FSH and LH levels but also helped maintain healthy testosterone levels. Fatima and Sultana [30] similarly reported favorable changes in estrogen and progesterone levels with various Ayurvedic formulations, while Devi et al. [29] observed improved hormonal balance with Sukumara Ghritam and Brahmi Churnam.
Dosage and duration
The dosage and duration of Ayurvedic herbal therapies play a crucial role in their efficacy for managing menopausal symptoms. Steels et al. [20] administered a daily dose of 500 mg of a combination of Tinospora cardifolia, Asparagus racemosus, Withania somnifera and Commiphora mukul for 12 weeks and found significant reductions in menopausal symptoms, including improvements in psychological and somatic domains. This suggests that a sustained treatment period with a moderate dosage may be necessary for optimal results. Gudise et al. [21] demonstrated the efficacy of Shatavari (Asparagus racemosus) at a daily dosage of 1 g over 8 weeks. This relatively shorter duration still resulted in significant improvements in hormonal levels and a reduction in hot flashes and night sweats, indicating the potency of Shatavari in managing menopausal symptoms.
Tomar et al. [28] investigated a combination therapy of Ashokarishta, Ashwagandha Churna and Pravala Pishti, with dosages ranging from 250 mg to 1 g daily over 6 months. The extended duration of treatment allowed for gradual but sustained improvements in hormonal balance and symptom severity, suggesting that long-term interventions may be beneficial for certain women. Gopal et al. [22] studied a novel fenugreek seed extract at a daily dosage of 500 mg over 12 weeks, demonstrating significant improvements in hormonal levels and menopausal symptoms. This consistent dosage and duration may provide a reference point for future studies investigating fenugreek’s efficacy.
Khanna et al. [23] explored the effects of a higher dosage of fenugreek seed extract (1,000 mg daily for 12 weeks) and found more pronounced improvements in hormonal balance and symptom relief, suggesting that higher dosages might be warranted in some cases. However, the potential risks associated with higher dosages need further investigation. Fatima and Sultana [30] and Devi et al. [29] examined Ayurvedic/ Siddha formulations with varying dosages, typically around 500 mg to 1 g daily, over 8 to 12 weeks, with positive outcomes in terms of hormonal balance and symptom reduction. This suggests a flexible yet effective dosage range for different formulations, emphasizing the importance of individualized treatment plans.
Risk of bias assessment
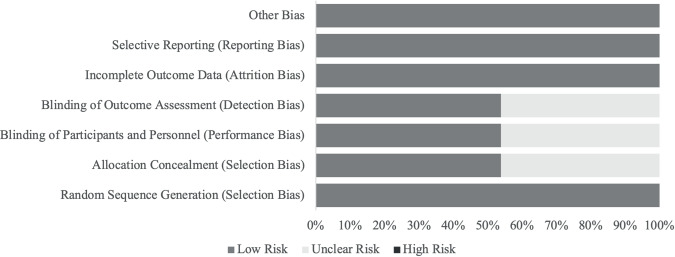
The risk of bias assessment for the 13 included studies was conducted using the Cochrane risk-of-bias tool for randomized trials (Figure 2). For the domain of random sequence generation (selection bias), all studies (100%) were rated as low risk. Allocation concealment (selection bias) showed a more varied risk, with 53.85% of studies rated as low risk and 46.15% as unclear risk. Similarly, blinding of participants and personnel (performance bias) was assessed as low risk in 53.85% of studies, with the remaining 46.15% rated as unclear risk. The domain of blinding of outcome assessment (detection bias) reflected the same distribution, with 53.85% low risk and 46.15% unclear risk. Incomplete outcome data (attrition bias) and selective reporting (reporting bias) were consistently rated as low risk across all studies, with 100% of studies falling into this category for both domains. Lastly, other potential sources of bias were also uniformly rated as low risk in 100% of the studies. This comprehensive assessment indicates a generally low risk of bias across most domains, with some uncertainty primarily in the areas of allocation concealment, blinding of participants and personnel and blinding of outcome assessment.
Discussion of the review results
The present systematic review consolidates evidence from 13 RCTs, highlighting the potential of Ayurvedic/Siddha interventions in effectively managing menopausal symptoms. These studies collectively emphasize the efficacy of diverse Ayurvedic herbal formulations, individual herbs and combined therapies in alleviating both somatic and psychological manifestations of menopause.
The study by Santwani et al. [19] serves as a cornerstone in this body of evidence, demonstrating that Saraswatarishta, a traditional Ayurvedic/Siddha formulation, provides significant relief from both somatic and psychological menopausal symptoms, comparable to HRT. This finding is particularly compelling given the growing concerns regarding the long-term safety of HRT and its association with increased risks of certain cancers [31]. The study’s methodology, employing a randomized controlled design, lends credence to the observed benefits of Saraswatarishta, positioning it as a potential alternative or adjunct therapy for menopausal women.
Further research has elucidated the effects of specific herbal constituents and their synergistic actions in multi-herb formulations. Steels et al. [20] demonstrated the efficacy of a formulation comprising Tinospora cardifolia, Asparagus racemosus (Shatavari), Withania somnifera (Ashwagandha) and Commiphora mukul (Guggul) in ameliorating vasomotor symptoms, musculoskeletal discomfort and psychological distress. The actions of these herbs, attributed to their diverse phytochemical profiles, may contribute to the formulation’s broad spectrum of benefits. This is consistent with the Ayurvedic/Siddha principle of employing multiple herbs with complementary actions to address the nature of menopausal syndrome [32].
Shatavari, a prominent herb in Indian traditional medicine, has emerged as a promising intervention for both psychological and somatic menopausal symptoms. The study by Gudise et al. [21] confirmed its efficacy in reducing anxiety, depression, hot flashes and insomnia in both pre- and postmenopausal women. This comprehensive effect may be attributed to Shatavari’s adaptogenic properties, which help the body cope with stress and restore hormonal balance. Moreover, the study’s robust design, employing a double-blind, multi-center RCT, strengthens the evidence for Shatavari’s therapeutic potential.
The psychological impact of menopause is a significant concern, and the reviewed studies provide compelling evidence for the efficacy of Ayurvedic/Siddha herbs in this domain. Santwani et al. [19] noted significant reductions in anxiety, depression and irritability with Saraswatarishta and Shirodhara, indicating the potential of these interventions in modulating neurotransmitter levels and promoting emotional well-being. Steels et al. [20] and Gudise et al. [21] further corroborated these findings, demonstrating significant improvements in depressive symptoms, quality of life, and psychological distress with their respective interventions. Additionally, Ashwagandha and fenugreek [22-25] have been shown to improve mood and emotional stability, suggesting their potential role in addressing the psychological challenges of menopause.
The safety and tolerability profile of Ayurvedic/Siddha herbal therapies is another important aspect highlighted in this review. Most studies reported minimal or mild adverse effects, indicating that these therapies are generally safe for most women. However, as highlighted by Khanna et al. [23], some interventions were associated with moderate adverse effects, underscoring the need for individualized assessment and careful monitoring.
The dosage and duration of interventions varied across studies, highlighting the need for further research to establish standardized protocols. While Steels et al. [20] demonstrated efficacy with a moderate dosage (500 mg daily) over 12 weeks, Gudise et al. [21] achieved positive outcomes with a higher dosage (1 g daily) over a shorter duration (8 weeks). These findings suggest that the optimal dosage and duration may vary depending on the specific herb or formulation, the individual’s constitution and the severity of symptoms.
The diverse mechanisms of action exhibited by herbs offer a multifaceted approach to menopausal symptom management. Shatavari, for instance, is renowned for its adaptogenic properties, which help the body adapt to stress and restore balance. This may contribute to its efficacy in reducing anxiety, depression and hot flashes by modulating the hypothalamic-pituitary-adrenal (HPA) axis and neurotransmitter levels [33]. Additionally, Shatavari’s estrogenic activity may play a role in alleviating hormonal imbalances and associated symptoms like vaginal dryness and decreased libido [34].
Ashwagandha, another prominent herb, exerts its effects through multiple pathways. Its adaptogenic and anxiolytic properties may help reduce anxiety and improve mood by interacting with GABA receptors and modulating cortisol levels [35]. Moreover, Ashwagandha’s anti-inflammatory actions may contribute to its benefits in reducing musculoskeletal discomfort and other inflammatory conditions often exacerbated by menopause [36].
The multi-herb formulation used by Steels et al. [20] harnesses the synergistic effects of various constituents. Tinospora cardifolia, known for its immunomodulatory and anti-inflammatory properties, help alleviate hot flashes and night sweats by reducing inflammation and modulating immune responses [37]. Commiphora mukul (Guggul), with its lipid-lowering and anti-inflammatory effects, may contribute to cardiovascular health and reduce the risk of atherosclerosis, a concern for menopausal women [38]. The combined actions of these herbs, along with Shatavari and Ashwagandha, may offer a comprehensive approach to addressing the physiological and psychological factors involved in menopause.
The appeal of Indian traditional medicine treatments extends beyond their pharmacological effects. Cultural and individual factors play a significant role in women’s preferences for these therapies. In many cultures, Ayurveda and Siddha are deeply ingrained in traditional healthcare practices and hold a revered position in promoting health and well-being [39]. The holistic approach of Ayurveda and Siddha, emphasizing the interconnectedness of mind, body and spirit, resonates with many women seeking personalized and natural approaches to health. Additionally, the emphasis on lifestyle modifications, dietary adjustments and individualized treatment plans aligns with the growing interest in preventive medicine and self-care [40].
Individual factors, such as personal beliefs, experiences with conventional medicine and cultural background, also influence preferences for Ayurvedic- and Siddha-based treatments. Women who have experienced adverse effects or dissatisfaction with conventional therapies may seek alternatives like Ayurveda and Siddha, which offer a gentler and more holistic approach. Furthermore, the cultural acceptability and familiarity with Ayurvedic practices in certain communities may contribute to their widespread use and acceptance [41].
Siddha medicine and menopause management
Like Ayurveda, Siddha medicine is a traditional Indian system of medicine with a holistic approach to health and well-being. Originating in ancient Tamil Nadu, Siddha medicine emphasizes the balance of three humors (vatha, pitta, and kapha) and utilizes various modalities, including herbal therapies, dietary recommendations and lifestyle modifications, to promote health and manage disease. While there is less research on Siddha medicine for menopause compared to Ayurveda, several studies included in this review provide insights into its potential benefits [41].
Devi et al. [29] investigated the effects of Sukumara Ghritam and Brahmi Churnam, two Siddha formulations, on menopausal symptoms. The study found significant reductions in physical discomfort and bodily sensations, as well as improvements in hormonal balance, after 8 weeks of treatment. These findings suggest that Siddha formulations may offer a viable option for managing somatic symptoms and restoring hormonal equilibrium in menopausal women.
The study by Fatima and Sultana [30] explored the use of Gokshura (Tribulus terrestris), an herb commonly used in Siddha medicine, for joint and muscular pain in menopausal women. The study reported a notable reduction in pain scores compared to the placebo group, highlighting the potential of Siddha herbs in addressing specific menopausal complaints. While these studies provide preliminary evidence for the efficacy of Siddha medicine in menopause management, further research is needed to explore its full potential. Future studies should investigate a wider range of Siddha interventions, including other herbal formulations, dietary recommendations and lifestyle modifications [9]. Additionally, comparative studies between Siddha and Ayurvedic therapies, as well as conventional treatments, would help elucidate their relative benefits and optimal applications for different individuals and symptom profiles.
The similarities between Siddha and Ayurvedic medicine, both rooted in ancient Indian traditions and emphasizing holistic approaches to health, suggest that they may offer complementary benefits for menopausal women. By integrating the knowledge and practices of both systems, healthcare providers can offer a more comprehensive and personalized approach to menopause management, catering to individual preferences and cultural backgrounds [9].
Strengths and limitations of the study
This systematic review offers a robust assessment of Ayurvedic interventions for menopausal symptom management, encompassing a diverse range of RCTs. The synthesis of evidence from multiple studies provides a comprehensive overview of the efficacy, safety and potential mechanisms of action of these interventions. The inclusion of studies with varying methodologies and interventions strengthens the review’s generalizability, while the rigorous assessment of risk of bias using the Cochrane RoB 2 tool ensures the methodological quality of the included evidence.
However, several limitations warrant consideration. The heterogeneity in study designs, sample sizes, intervention protocols and outcome measures introduces variability, potentially hindering direct comparisons between studies. The reliance on subjective outcome measures, such as self-reported symptom severity and quality of life assessments, may introduce potential bias. Furthermore, the predominance of single-center studies and limited geographical diversity of study populations raise concerns about the generalizability of findings to broader populations. These limitations highlight the need for future research to address these methodological gaps and provide more definitive conclusions.
Implications: clinical and policies
Clinical implications
The findings of the systematic review hold significant implications for the practice of Complementary and Alternative Medicine (CAM) in the context of menopause management. As women increasingly seek holistic and personalized approaches to address menopausal symptoms, Ayurvedic and Siddha herbal therapies emerge as promising alternatives or adjuncts to conventional HRT, which may be associated with adverse effects or contraindications [42]. The evidence presented in this review demonstrates that Ayurvedic and Siddha interventions can effectively alleviate both physical and psychological symptoms of menopause. Notably, the significant reduction in vasomotor symptoms like hot flashes and night sweats observed across multiple studies suggests a potential role for these therapies in improving quality of life and reducing reliance on pharmaceutical interventions [15,16,18]. Furthermore, the positive impact on psychological well-being, evident in the reduction of anxiety, depression and mood swings [14-16], highlighting the holistic nature of these treatments, aligning with the growing emphasis on the mind-body connection in health and disease management.
The findings provide healthcare providers with an opportunity to expand their therapeutic toolkit and offer more comprehensive, patient-centered care. By integrating Ayurvedic and Siddha principles and practices into their approach, practitioners can provide women experiencing menopause with a wider range of personalized treatment options that cater to individual needs and preferences. This shift towards integrative medicine aligns with the increasing demand for natural and holistic health solutions. However, the integration of Ayurvedic and Siddha therapies into mainstream healthcare requires addressing several challenges [43]. The lack of standardized protocols and guidelines for their use in menopause management necessitates further research to determine optimal dosages, durations and combinations of herbs and formulations for specific symptom profiles and individual constitutions. Additionally, rigorous clinical trials with larger, more diverse populations are needed to further validate the safety and efficacy of these therapies and investigate potential interactions with conventional medications. Despite these challenges, the potential benefits of Ayurvedic and Siddha herbal therapies for menopausal women cannot be overlooked. Through collaboration between traditional medicine practitioners and conventional healthcare providers, coupled with robust research and the development of evidence-based guidelines, the integration of these therapies into routine clinical practice can become a reality [44]. This integrative approach can bridge the gap between traditional wisdom and modern medicine, providing women with a more comprehensive and holistic approach to menopause management.
Policy implications
Given the growing global interest in and utilization of Ayurvedic and Siddha medicine, there is a compelling need for supportive policies and regulations to ensure their safe and effective integration into healthcare systems. The Ministry of AYUSH (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy), established by the Government of India, is uniquely positioned to lead this effort. The Ministry of AYUSH has already demonstrated its commitment to promoting and regulating these traditional medicine systems. It has established research institutions, like the Central Council for Research in Ayurvedic Sciences (CCRAS), to investigate the efficacy and safety of Ayurvedic interventions [45]. It has also undertaken the standardization of herbal drugs to ensure quality and consistency, and it has developed educational and training programs for practitioners to maintain high standards of practice.
However, more can be done to specifically address the needs of women experiencing menopause.
Building upon its existing initiatives, the Ministry can take several additional steps:
– Developing evidence-based guidelines: There is a need to create evidence-based guidelines for the use of Ayurvedic and Siddha therapies in menopause management. Such guidelines could provide healthcare providers with clear recommendations on the selection, dosage and duration of treatment, based on the latest research findings [46]. This would enhance the credibility of these therapies, facilitate their integration into mainstream healthcare and promote their safe and effective use.
– Fostering collaboration: Building a path of collaboration between Ayurvedic and Siddha practitioners and conventional healthcare providers is essential for creating a truly integrative approach to menopause care [47]. This can be achieved through joint research initiatives, educational programs and clinical collaborations. Such partnerships would not only enhance knowledge exchange but also contribute to developing more comprehensive and personalized treatment plans for women.
– Raising public awareness: There is still a need to increase the awareness level among the population. The Ministry of AYUSH could position itself to raise public awareness about the potential benefits of Ayurvedic and Siddha therapies for menopausal women. Through public education campaigns, outreach programs and media initiatives, women can be empowered to make informed decisions about their health care and explore the diverse options available to them [42]. This can lead to increased utilization of these therapies, broader acceptance within the medical community and, ultimately, improved quality of life for menopausal women.
– Regulatory framework: Further strengthening the regulatory framework for Ayurvedic and Siddha medicines would ensure quality control, safety and efficacy. This includes stricter regulations on the manufacturing and marketing of herbal products, as well as robust pharmacovigilance systems to monitor adverse events and ensure patient safety.
– Research funding: Moreover, encouraging health researchers by allocating more funding for research on Ayurvedic and Siddha interventions for menopause would generate high-quality evidence and expand the knowledge base. This would facilitate the development of standardized treatment protocols and enhance the credibility of these therapies among healthcare providers and the public.
By addressing these areas, the Ministry of AYUSH can play a pivotal role in integrating Ayurvedic and Siddha medicine into the mainstream healthcare system, providing women with safe, effective and accessible options for managing menopausal symptoms. This would not only benefit individual women but also contribute to the overall well-being of society by promoting a more holistic and personalized approach to health care.
Conclusions
In conclusion, this systematic review supports the potential of Ayurvedic and Siddha interventions in managing menopausal symptoms. The evidence suggests that these therapies can effectively alleviate physical and psychological complaints, modulate hormonal levels and enhance overall well-being. However, the heterogeneity and methodological limitations of the included studies necessitate the need for further research to confirm these findings and establish definitive guidelines for clinical practice.
Future research should prioritize large-scale, multicentre RCTs with standardized interventions and outcome measures [48]. Additionally, investigating the long-term effects and optimal dosages of Ayurvedic and Siddha therapies, as well as exploring the synergistic effects of combined interventions, are crucial areas for future investigation [49]. By addressing these research gaps, we can enhance our understanding of the role of Ayurvedic and Siddha medicine in menopause management and facilitate their integration into evidence-based clinical practice.
Disclosures and acknowledgements
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Artificial intelligence (AI) was not used in the creation of the manuscript.