Introduction
Gestational diabetes mellitus (GDM) is a common metabolic condition identified by glucose intolerance that emerges for the first time during pregnancy [1]. It poses significant health risks for both mothers and their offspring, contributing to adverse pregnancy outcomes and increasing the likelihood of long-term metabolic complications [2]. The etiology and genetic foundations of GDM are not yet fully elucidated, prompting intensive research efforts to identify modifiable risk factors that could inform preventive strategies [3,4].
Among the numerous factors implicated in the pathogenesis of GDM, lifestyle behaviors have garnered considerable attention due to their potential for [5]. Amidst the myriad factors influencing GDM development, physical inactivity, characterized by insufficient regular exercise and sedentary behaviors, emerges as a modifiable lifestyle factor warranting thorough examination [6].
The American College of Obstetrics and Gynecology (ACOG) recommends that pregnant women should engage in at least 150 minutes of moderate-intensity aerobic activity throughout the week, which can be broken down into approximately 30 minutes of exercise on >5 days/week in case of no contraindication [7,8].
Aerobic exercise and resistance training are considered some of the safest and most effective forms of exercise for preventing gastrointestinal motility disorders [9,10].
In contemporary societies, sedentary lifestyles have become increasingly prevalent, driven by technological advancements, urbanization, and changing work patterns [11]. As a result, prevalence of physical inactivity among pregnant women is on the rise, raising concerns about its potential contribution to the escalating rates of GDM worldwide [8,12].
Physical activity (PA) reduces GDM risk through protective effects, enhancing glucose uptake in muscles and decreasing insulin resistance, which is crucial during pregnancy when insulin resistance naturally increases [5]. The effects are primarily mediated by improved insulin sensitivity via GLUT4 translocation, increasing glucose uptake by muscle cells, improving mitochondrial function and fatty acid oxidation, enhances endothelial function [13-16]. Regular exercise reduces inflammatory markers, including C-reactive protein (CRP) and interleukin-6 (IL-6), helping to lower diabetes risk [17,18].
While the beneficial effects of regular PA on metabolic health are well-established in the general population, its specific impact on GDM risk during pregnancy warrants further investigation for devising effective preventive strategies and optimizing maternal and fetal health outcomes [19].
Several observational studies have reported associations between physical inactivity and an increased likelihood of developing GDM. However, the evidence remains heterogeneous, with variations in study designs, population characteristics, and measures of PA complicated interpretation [20].
The multifactorial nature of GDM necessitates a meticulous investigation into the interplay between physical inactivity and other established risk factors, such as age, body mass index, dietary habits, and genetic predispositions. The review uses a systematic approach to delineate the independent contribution of physical inactivity toward GDM onset while discerning potential synergistic or mitigating effects in conjunction with other risk factors.
Ultimately, synthesizing the existing evidence on the association between physical inactivity and GDM will provide clinicians, public health policymakers, and expectant mothers with valuable insights to guide preventive measures and interventions. By elucidating the significance of PA in mitigating the GDM risk, the review endeavors to contribute to the optimization of maternal health and the reduction of adverse pregnancy outcomes.
Aim of the work
The review aims at exploring the role of physical inactivity in the development of GDM by analyzing evidence from diverse study designs.
Methods
Search strategy
Literature searches were conducted using the databases MEDLINE, Scopus, CINAHL, Embase, and Cochrane Library from March 2009 to March 2024, with an update in August 2024. We used various keyword combinations to account for different search parameters in each database: (“pregnancy” OR “gestation” OR “gestational” OR “maternal” OR “antenatal”) AND (“exercise” OR “activity” OR “PA” OR “physical exercise”) AND (“gestational diabetes” OR “GDM” OR “insulin sensitivity” OR “glucose tolerance” OR “diabetes mellitus” OR “diabetes”). Additionally, bibliographies of relevant articles were examined to ensure a comprehensive collection. Three reviewers independently analyzed and selected potential studies identified through the search strategy.
Study selection
Only human studies published in English were considered. We focused on studies involving pregnant women in their first trimester. Studies were excluded if they involved participants at low risk of GDM, those with pre-existing diabetes, high-risk pregnancies, or if they were not conducted in routine care settings. There were no exclusions based on various international definitions of GDM.
Quality assessment
We used the Mixed Methods Appraisal Tool (MMAT) to assess the quality of the original studies. The MMAT was initially developed in 2006 and revised in 2011 [21]. The tool allows for the concurrent appraisal and description of methodological quality in case-control, cohort, and cross-sectional studies. For our assessment, we used section 3 of the MMAT to evaluate the study quality. Each item is marked as yes, no, and cannot tell. The total number of items rated “yes” is counted to produce an overall score. The score is determined by the number of criteria met divided by four, resulting in a range from 25% (*) for one criterion met to 100% (****) for meeting all criteria [21-23].
Literature review results
Identified studies
A comprehensive search across multiple databases initially identified 120 potentially relevant papers. After screening titles and abstracts and removing duplicates, we retrieved full texts of 50 papers for further review. Following applying various exclusion criteria, we excluded several studies, including one where the author failed to provide additional methodological details. In the end, 12 studies (as shown in Table 2) met the inclusion criteria for the synthesis [20,24-33]. The process of study selection is depicted in Figure 1.
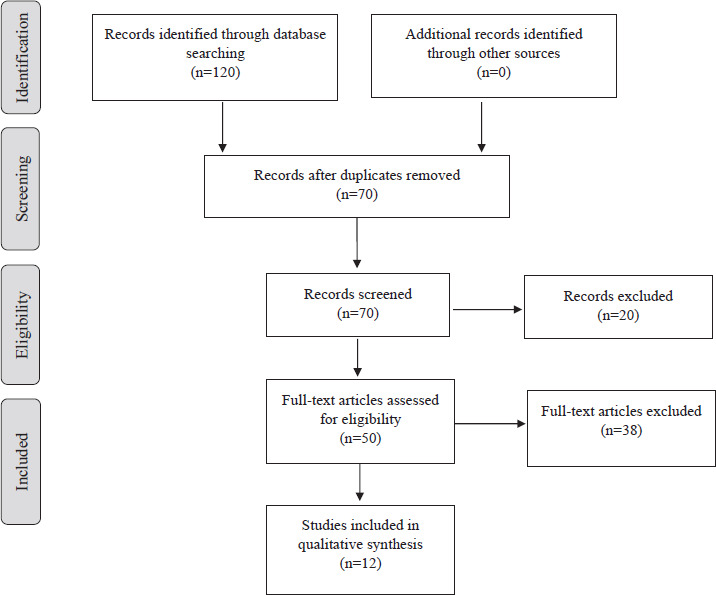
Table 1
Study characteristics
| Study number | Author(s) and year | Study design | Population | Sample size | PAassessment | Diagnostic criteria | Results |
|---|---|---|---|---|---|---|---|
| 1. | Ramos-Levi et al., 2012[26] | Cohort study | Pregnant women in Spain | 2,194 | Questionnaire | Carpenter and Coustan’s criteria | Light walking (>30 minutes/day) and sports activities (≥2 days/ week) reduce the chanceof GDM. |
| 2. | Li et al., 2013 [33] | Cross-sectional | Pregnant women in Guangzhou, China | 571 | IPAQ | IADPSGcriteria | 13% of the women had GDM, associated with increased intake of local foods and lower PA levels (≤600 MET-min /week). |
| 3. | Badon et al., 2017 [20] | Cohort study | Pregnant women in Washington,the USA | 3,005 | Questionnaire | American DiabetesAssociationguidelines | PA (>3 METs) reduced the risk of GDM by 21% for each 1-point increasein lifestyle score. |
| 4. | Ramos do Nascimento et al., 2019[31] | Cross-sectional | Low-income pregnant women in Brazil | 544 | PPAQ | IADPSGcriteria | GDM occurred in 17.4% of participants, among which 61.0 % were physically inactive (<1.5METs). |
| 5. | Leng et al., 2016 [30] | Cross-sectional | Pregnant women in Tianjin, China | 11,450 | Questionnaire | IADPSGcriteria | Extended periods of sitting were markedly linked to a heightened likelihood of developingGDM. |
| 6. | Amiri et al., 2016 [27] | Case-control | Pregnant women in Babol, Iran | 200 | PPAQ | Carpenter and Coustan criteria | GDM was more prevalent in women with low total PA, as compared to those with higher PA levels (activities with MET >3MET). |
| 7. | Chasan-Taber et al., 2010[25] | Cohort study | Hispanic women in Massachusetts, the USA | 632 | PPAQ | American DiabetesAssociation criteria | 18.7% of participants met the guidelines for PA before pregnancy, while 5.2% met these guidelines in earlypregnancy. |
| 8. | Mørkrid et al., 2014 [34] | Cohort study | Pregnant women in Oslo, Norway | 759 | Sense Wear™ Armband | IADPSGcriteria | 30% of women with GDM reported engaging in regular PA before pregnancy, as compared to 44% of those withoutGDM. |
| 9. | Mishra et al., 2020 [32] | Case-control | Pregnant women in Karnataka, India | 373 | IPAQ | Carpenter and Coustan criteria, later switched toDIPSI criteria | Total PA <600 MET-minutes/week isa significant risk factor for GDM. |
| 10. | Retnakaran et al., 2009[24] | Obser-vational cohort study | Healthy pregnant women in Canada | 851 | Baecke questionnaire | GCT and OGTT | Women with glucose tolerance were engaged in higher levels of vigorous/sports activity before pregnancy than those with abnormalglucose tolerance. |
| 11. | Anjana et al., 2016 [28] | Case-control | Pregnant women in Chennai, India (GDM cases andcontrols) | 795 | MPAQ,pedometer | IADPSGcriteria | Sedentary behavior increased the likelihood of GDM four times, whereas walkingreduced GDM by 70%. |
| 12. | Badon et al., 2016 [29] | Cohort study | Pregnant women in Washington State, theUnited States | 3,209 | LTPA | Carpenter and Coustan’s criteria | High LTPA duration before pregnancy (6-32.5 hrs/wk), lowers the risk of GDM by 45%. |
[i] Notes: IADPSG – The International Association of Diabetes and Pregnancy Study Groups, GCT – Glucose Challenge Test, OGTT – Oral Glucose Tolerance Test, DIPSI – Diabetes in Pregnancy Study Group India, MPAQ – Madras Diabetes Research Foundation – Physical Activity Questionnaire, IPAQ – International Physical Activity Questionnaire, PPAQ – Pregnancy Physical Activity Questionnaire, LTPA – Leisure-Time Physical Activity.
Table 2
Quality assessment
| Study number | Study | Representative participants | Appropriate measurements | Confounding factors controlled | Complete follow-up | Exposures administered as intended | Overall score | Quality of the study |
|---|---|---|---|---|---|---|---|---|
| 1. | Badon et al., 2016 [29] | Yes | Yes | Yes | Notmentioned | Yes | 80% | Moderate to High-QualityStudy |
| 2. | Retnakaran etal., 2009 [24] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 3. | Anjana et al.,2016 [28] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 4. | Ramos-Levi etal., 2012 [26] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 5. | Badon et al.,2017 [20] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 6. | Ramos do Nascimento etal., 2019 [31] | Yes | Yes | Yes | Yes | Yes | 100% | High-Quality Study |
| 7. | Leng et al.,2016 [30] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 8. | Amiri et al.,2016 [27] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 9. | Chasan-Taber et al., 2010[25] | Yes | Yes | Yes | Yes | Yes | 100% | High-Quality Study |
| 10. | Mørkrid et al.,2014 [34] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 11. | Mishra et al.,2020 [32] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
| 12. | Li et al., 2013[33] | Yes | Yes | Yes | Yes | Yes | 100% | High-QualityStudy |
Study characteristics
We individually selected the research works included in the synthesis, considering the eligibility criteria. The included studies explored the relationship between PA and GDM across diverse populations, employing various assessment methods. The studies were conducted in eight countries: the USA, Norway, India, Iran, China, Brazil, Canada, and Spain (Table 1). Most papers were cohort studies, with three being case-control and three being cross-sectional. All the studies included pregnant women, both with and without GDM, comprising a total of 24,583 participants. Most of the research used different questionnaires to assess PA (Table 2), with only two studies utilizing pedometers and armbands in addition to questionnaires [28,34]. Different criteria used for the GDM diagnosis are mentioned in Table 1.
Methodological quality
The studies’ quality was assessed using the MMAT, which recommended one moderate-quality study and eleven high-quality studies (Table 2). Any disagreement was resolved by collaborative deliberation.
PA during pregnancy
To date, three observational studies have analyzed the relationship between pre-pregnancy PA levels and glucose and insulin metabolism during pregnancy. Pregnant women from Norway were studied to find the link between pre-pregnancy PA measured objectively and GDM. Interestingly, only 30% of women with GDM reported engaging in regular PA before pregnancy, as compared to 44% of those without GDM [34]. One research focused on PA types and metabolic parameters during pregnancy. Glucose intolerance decreased with a higher level of pre-pregnancy total PA (p=0.024). Women with standard glucose tolerance reported significantly higher levels of vigorous/sports activity before pregnancy than those with abnormal glucose tolerance (p=0.004) [24]. Additionally, a prospective cohort study among Hispanic women in Massachusetts evaluated PA, psychosocial stress, and GDM risk, finding that 18.7% of participants met the guidelines for PA before pregnancy, while 5.2% met the guidelines in early pregnancy (30 minutes of moderate PA on >5days/week) [25].
Two studies have objectively measured PA levels to examine their association with glucose intolerance in pregnancy. One case-control study involving 795 pregnant women used pedometers and a questionnaire to assess PA status. The results demonstrate that women with GDM exhibit significantly higher levels of sedentary behavior, as compared to women without the condition (86.2% vs. 61.2%; p<0.001). Sedentary behavior demonstrated a significant fourfold increase in the likelihood of adverse outcomes, whereas engaging in recreational walking was linked to a notable 70% reduction in the risk of GDM [28]. The study conducted by Morkrid et al. [34] utilized armbands to monitor PA during early gestation. Women diagnosed with GDM were found to take fewer steps on average per day (Mean 7964 steps/day) and engage in moderate intensity of PA (3-6 METs; p<0.005), as compared to women without GDM [34].
Three observational researches have evaluated the effect of PA during pregnancy on GDM development. Authors used the questionnaire to assess PA levels in early pregnancy and found that GDM was more prevalent in women with low total PA (p=0.001), as compared to those reporting higher PA levels (activities with MET >3 MET) [27]. A study in China examined the relationship between dietary habits, PA, and cognitive factors with GDM risk, finding that 13% of the women had GDM, associated with increased intake of local foods and lower PA levels (≤600 MET-min/week) [33]. In Karnataka, India, pooled data identified physical inactivity (total PA <600 MET-min/week) as a significant risk factor for GDM (adjusted OR: 21.0; p=0.003) [32].
A cross-sectional and cohort study involving 11,450 pregnant women in China and 3,005 women in Washington supported the findings. Women with GDM were more likely to be engaged in less than three hours of LTPA and less than one hour of household work. Pregnant women diagnosed with GDM demonstrated a reduced propensity to participate in moderate to vigorous PA during their pregnancy (79.8% vs. 81.6%; p=0.191) [30]. In Washington, adherence to a healthy lifestyle, including PA (>3 METs) reduced the risk of GDM by 21% for each 1-point increase in lifestyle score [20]. Additionally, a cohort study from Spain found that light walking (>30 min/day) and sports activities (≥2 days/week) reduce the chances of GDM [26]. One study investigated LTPA and its association with GDM risk, finding that if LTPA duration before pregnancy is high (6-32.5 hrs/wk), it lowers the risk of GDM by 45% [29].
In Brazil, a study of 544 low-income pregnant women found that GDM occurred in 17.4% of participants, among which 61.0% were physically inactive (<1.5 METs) [31]. Cumulative results suggest that engaging in PA before and during the early stages of pregnancy is correlated with a decreased likelihood of GDM development, with the most robust protective impact noted in women who were physically active before conception.
Discussion of the review results
The findings of the systematic review provide a comprehensive assessment of the PA as a risk factor for GDM. The evidence underscores the potential benefits of PA as a preventive measure for GDM but also highlights the complexity and variability in outcomes across different studies. The effectiveness of PA programs in controlling GDM was mentioned in a systematic review [35], whereas another systematic review and meta-analysis revealed a curved pattern of influence between activity done before pregnancy and the risk of GDM [9]. Our findings align with the broader literature highlighting the beneficial effects of PA on overall metabolic health [6]. The relationship between PA and GDM is crucial, as highlighted by those who discussed the association between physical inactivity and mortality due to diabetes mellitus [36]. Furthermore, physical inactivity is also a leading risk factor for various health conditions, including GDM [37]. A meta-analysis revealed a significant association between elevated PA levels before pregnancy and a reduced likelihood of developing GDM [9]. Activities performed before pregnancy seem to have a more pronounced protective effect, as compared to those initiated during pregnancy. It may be due to the establishment of better metabolic health before pregnancy [38]. The importance of lifestyle modifications, including PA, in improving outcomes for women with GDM was underscored in another study [39]. Increased sedentary time, regardless of PA levels, is also associated with a higher risk of GDM. It suggests that reducing sedentary time is as important as promoting PA [30]. Low income was identified as a contributing factor to physical inactivity among females, which subsequently increases the risk of developing GDM [31]. In conclusion, physical inactivity plays a significant role in the development and management of GDM. Incorporating PA interventions in the care of pregnant women can potentially reduce the risk of GDM and improve maternal and child health outcomes.
Despite the overall positive association, the review highlighted significant heterogeneity in the outcomes of the studies. Self-reported PA data could be susceptible to recall bias. Future research should consider using objective measures of PA, such as accelerometers, to validate the findings. Standardizing the measurement of PA and sedentary behavior will improve comparability across studies. Variations in study designs, population characteristics, and PA assessment methods contribute to inconsistent findings. For example, while some studies reported a substantial risk reduction, others found minimal effect. Additionally, longitudinal studies tracking PA patterns from preconception through postpartum would provide valuable insights into the timing and duration of activity needed to confer protective effects.
Conclusions
PA holds promise as a modifiable risk factor for GDM, with evidence supporting its role in prevention. However, variability in findings necessitates further research to refine recommendations and develop effective intervention strategies tailored to diverse populations.
Disclosures and acknowledgments
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Artificial intelligence (AI) was not used in the creation of the manuscript.