Introduction
According to the WHO, depression causes the death of over 700,000 people every year [1]. Women are twice as likely to be ill, and a significant proportion of them become ill during pregnancy or the postpartum period. Postpartum depression is the second cause of suicide death between pregnancy and a year after childbirth, and 1 in 7 women who take their own lives does so between six weeks and a year after giving birth [2]. Although official statistics may be underestimated, it is estimated that as many as 48,000 to 73,000 women in Poland may suffer from postpartum depression [3].
The American Psychiatric Association (APA) reports that there is a strong link between childbirth and the occurrence of mood disorders. Due to the dynamics of biological, psychological and sociocultural changes, the puerperium is the period of greatest vulnerability of a woman to psychological disorders, throughout her life [4]. Hopkins et al. [5] detailed three types of postpartum emotional distress. Depending on the symptoms and their severity, we distinguish between postpartum blues (or baby blues), postpartum depression (PPD) and postpartum psychosis. The most common of these is postpartum blues characterized by a temporary and moderate lowering of mood, emotional vacillation, tearfulness, exhaustion, and a decrease in appetite. Postpartum blues appears in the first two weeks of the puerperium and usually subsides on its own. Sadness and feelings of overwhelm of greater intensity, lasting for most of the day, accompanied by anxiety, guilt, lack of feelings of joy and pleasure, sleep disturbances and even the appearance of suicidal thoughts, may already indicate the presence of PPD. An extreme condition is postpartum psychosis, which is characterized by inadequate reception and perception of reality, often resulting from delusions, causing significant dysfunction. Visual and auditory hallucinations can lead a mother to harm herself or her child. As a life-threatening condition, psychosis requires urgent intervention, stabilization of the woman’s mental state and protection of the newborn [5]. Postpartum psychosis is very rare, occurring in 0.1-0.2% of puerperae. PPD is estimated at 6.5-20%, while postpartum blues is estimated at up to 40-80% [6]. However, these data may be significantly underestimated due to unreliable diagnostics. Medical personnel often mistakenly perceive the first symptoms of depression as physiologically occurring emotional lability in women after childbirth [3].
In response to the growing problem of emotional disorders in women during the perinatal period in Poland, a “Program on education and prevention of PPD” has been developed for 2018-2023, aimed at increasing the percentage of women with early diagnosis of PPD through education and increasing awareness about it, both among medical staff and women themselves. No institution from the Lesser Poland Voivodeship joined the program [7]. In 2019, standards for perinatal care were introduced (and maintained in the 2023 standards), according to which women’s emotional state, in terms of risk of mood disorders, should be assessed three times, twice during pregnancy and then in the puerperium [8]. Despite the introduction of standards, medical staff have not been trained for this purpose. To assess the mental state of puerperae, midwives use a non-standardized interview method, for which, according to a study by Chrzan-Dętkoś and Walczak-Kozłowska [3], they are mostly unprepared. Midwives underestimate the problem of PPD, do not know its effects, and believe that medical help is not necessary in this area because the disorder is temporary and passes in a few days after hospitalization [3]. Meanwhile, research shows that PPD is not only a serious condition, often life-threatening for the mother, but can also significantly affect the deterioration of the mother-child relationship, as well as the child’s development. Mothers with PPD fail to make eye and body contact with their child, neglect care, and fail to attend scheduled follow-up appointments and vaccinations. Children of mothers with PPD show slower weight gain and slower growth rates [9].
Mood disorders in mothers can occur regardless of the type of birth. However, studies indicate that depression is more common in women after Cesarean section (CS) [10]. On a European scale, Poland, along with Cyprus and Hungary, is among the countries with the highest percentage of surgical deliveries, reaching as much as 44.4% [11]. Puerperae after CS, compared to those after vaginal birth (VB), have greater functional limitations, mainly during mobility and hygiene activities [12]. The cause is pain and perioperative complications, much more frequent after CS than after VB. The incision made during CS involves several layers of tissue, which are susceptible to the appearance of pain during the healing and regeneration process. In addition, contractions accompanying uterine involution and contractions stimulated by breastfeeding contribute to pain, and postoperative discomfort is compounded by the presence of intestinal gas and constipation [13].
Despite a better understanding of pain mechanisms, the introduction of modern analgesics and anesthetic techniques, the level of postoperative pain relief in European countries is still unsatisfactory. Ineffective pain control may lead to immunosuppression, infections and poor wound healing. Pain also prolongs the time of immobilization, which in turn may result in thrombosis and embolism, to which women after childbirth are particularly vulnerable. Furthermore, 9.2-18% of women develop chronic pain syndrome from acute postoperative pain, which in turn increases the amount of pain medication taken, including opioids [14]. Pain can also hinder the initiation of breastfeeding by blocking the release of oxytocin and impair the ability to optimally care for the baby in the immediate postpartum period. This may adversely affect early interactions between the mother and the newborn – making it difficult to establish a bond [15].
The meta-analysis by Moameri et al. [16] suggest several mechanisms explaining the association between CS and PPD. The increased risk of depression after surgical delivery compared to VB is due to biological changes in the mother’s body, increased risk of hemorrhage, increased neonatal mortality, breastfeeding failures. One of the reasons may also be the fact that women with a tendency to depression are a group that more often decides on surgical delivery due to increased fear of VB [16]. Regardless of whether the surgical termination of pregnancy is the woman’s choice or dictated by objective medical indications, it is associated with a higher risk of complications. After CS, women are immobilized for longer, undergo later verticalization, take more painkillers, and thus are unable to independently care for the child for a longer period of time. They are also more likely to have difficulties with breastfeeding. All these factors influence the first contact with the newborn and the mother’s emotions [17].
The finding that CS is more predisposing to PPD is disputed by some authors. Lim et al. [18] found no effect of type of delivery on the incidence of depression, demonstrating that it is not the type of tissue damage but the experience of pain itself that is a risk factor for emotional disturbance, suggesting that the level of pain severity in the postpartum period may influence the incidence of postpartum mood disorders.
Aim of the work
The aim of this study was to investigate whether pain levels in women after CS are related to the risk of depression in the immediate and late postpartum period.
Material and methods
The study was carried out in the Department of Gynecology and Obstetrics of the Specialized Hospital in Kraków, Poland. The study included 84 women on the first day after elective CS who gave birth to healthy newborns (Apgar score ≥8 points). In all the subjects, CS was performed using the Misgav-Ladach method, under epidural and/or spinal anesthesia. All the patients received the same pain medication regimen after surgery. Women whose pregnancy was at risk, patients with diagnosed mental disorders and/or tokophobia and puerperae with perinatal complications were excluded from participation in the study.
The puerperae were randomly allocated to one of two groups. In group A (n=50), physiotherapy was carried out to reduce pain (including a 20-minute pre-verticalization exercise program consisting of breathing techniques combined with forced expiration exercises and instruction on wound protection, circulation-stimulating, stretching and isometric exercises, mobilization of lumbosacral connective tissue; as well as instruction on how to perform these exercises during the first days of puerperium); group B (n=34) comprised patients under the care of midwives who did not receive postoperative physiotherapy.
A pain assessment was carried out using the Numerical Rating Scale (NRS), as recommended by the Polish Association for the Study of Pain. The level of pain experienced is determined on a scale of 0-10, where 0 means no pain and 10 means the most severe pain imaginable. Scores 1-3 describe mild pain, 4-6 moderate pain, 7-8 severe pain, 9-10 very severe pain [19].
Patients were asked to rate the severity of their pain sequentially at 7, 12 and 24 hours after the procedure. Seven hours after the procedure, patients were additionally asked about their comfort level. An 11-point NRS scale (where 0 means no comfort and 10 its highest level) was also used for this purpose. The Edinburgh Postnatal Depression Scale (EPDS) was used to assess postpartum mood disorders.
It is a screening test for the initial detection of the risk of the presence of postpartum depression. The questionnaire has undergone psychometric validation in the Polish language version [20]. The EPDS consists of 10 questions, with score of 0-3 available for answering each question. The overall score of the scale is obtained by adding up the points of the questionnaire, and the patient can obtain a maximum score of 30. For the Polish version of the scale, a score of 12 is considered the cut-off point. A score as low as 9 can already indicate a moderate risk of postpartum depression. An affirmative answer to the last question, regarding suicidal thoughts, even with a total score below 9, requires consultation with a mental health specialist. Patients were asked to complete the EPDS on the second day after CS as well as being given a second copy of the questionnaire, with a request to complete and return 4-6 weeks after delivery.
Statistical elaboration of the results
A descriptive analysis of sociodemographic data and obstetric characteristics was conducted. Data are presented using mean (M), minimum (Min) and maximum (Max) values, and standard deviation (SD). Statistical analysis was carried out using the STATISTICA 13 v.1 software. The normality of the distribution of the variables was checked using the Shapiro-Wilk test. The Mann Whitney U test for independent samples was used to compare between groups, while the Spearman’s rank correlation coefficient was used to calculate correlations. Test values and coefficients at the p<0.05 level were considered statistically significant.
Results
The study was conducted in a group of 84 women after CS. Descriptive characteristics are shown in Table 1.
Table 1
Characteristics of respondents
Level of pain and comfort of puerperae after CS
When measured 7 hours after CS, the mean pain level was 2.24 and 2.76 in groups A and B, respectively, and was not significantly different (p=0.109). In subsequent measurements – after 12 and 24 hours – the average pain declared by the puerperae in group A was 3.44 and 2.04, while in group B it was higher – after 12 hours – 4.09, after 24 hours – 3.29. The differences in measurements after 12 hours as well as after 24h were statistically significant (p=0.018 and p=0.000). In contrast, comfort levels at 7 hours after CS in group A ranged from 2 to 7 points, with the highest number of puerperae declaring a comfort level of 5 points. In group B, the maximum value in the patients’ assessment was 5, and the highest percentage declared a comfort level of 4. Comfort levels differed significantly between groups (p=0.000). Furthermore, an inverse high correlation was found between patients’ declared pain and comfort levels after 7 hours (p=0.000, r=-0.73). Details of pain and comfort levels by group are shown in Table 2.
Table 2
Level of comfort and pain in subsequent measurements after CS
Risk of postpartum depression
The mean score on the EPDS questionnaire in all subjects at the in-patient stage was 8.75 and differed significantly between groups (in group A the mean was – 8.32, in group B – 9.88; p=0.007). A total of 49 women (58.3% of subjects) were found to be at risk of depression (score of 9 or more), of which moderate risk (9-11 points) was found in 39 women (46.4%), while significant risk (12 points or more) was found in 10 subjects (11.9%). In groups A and B, the risk of depression was 50 and 70.6%, respectively. With group A showing a significant risk in 6% of puerperae, while group B showed a significant risk in 20.6%. The detailed distribution of results is shown in Table 3.
Table 3
Distribution of EPDS scores by group during hospitalisation
In a repeat test using the EPDS questionnaire, four to six weeks after CS, the mean was lower both for all subjects – 8.24 and for the individual groups – 7.79 in group A and 9.1 in group B. Only 29 women completed the questionnaire twice, representing 34.5% of all subjects. The differences between the groups were not statistically significant (p=0.126). The percentage of women showing an increased risk of depression in the whole group, decreased slightly – from 58.3% at hospitalization to 55.2% after 4-6 weeks. In group A, it decreased from 50% at hospitalization to 47.4% after 4-6 weeks, while in group B it decreased from 70.6% to 70%. It is noteworthy, however, that of the 49 puerperae at increased risk of depression, only 11 completed the questionnaire again. The detailed distribution of results in each group is shown in Table 4.
Table 4
Distribution of EPDS scores by group at 4-6 weeks after CS
Considering only the 29 subjects who completed the questionnaire twice, none of the groups showed a significant change in the EPDS score on repeat testing (p=1.0 and p=0.722, in groups A and B, respectively). It is noteworthy, however, that in the 3 puerperae who showed a significant risk of depression in the first survey, the outcome decreased to the moderate risk range. In contrast, of the 18 puerperae with a score from the first measurement that did not indicate a risk of depression, seven had values that increased to a level representing a moderate risk. A detailed distribution is shown in Table 5.
Table 5
Distribution of EPDS scores 4-6 weeks after delivery, according to scores at hospitalization (includes only respondents who completed the questionnaire twice; N=29)
| Late puerperium Early puerperium | x<9 n=13 | x=[9,10,11] n=15 | 12≤x n=1 |
|---|---|---|---|
| x<9n=18 | 11 | 7 | 0 |
| x=[9,10,11]n=8 | 2 | 5 | 1 |
| 12≤xn=3 | 0 | 3 | 0 |
There was a significant correlation between pain levels at 7, 12 and 24 hours after CS and the EPDS questionnaire score, as shown in Figures 1-3.
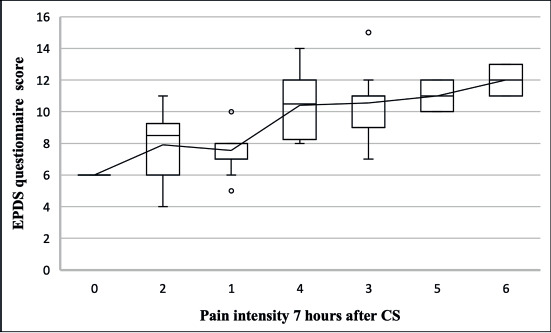
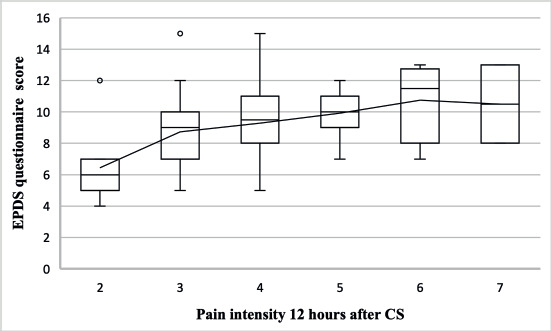
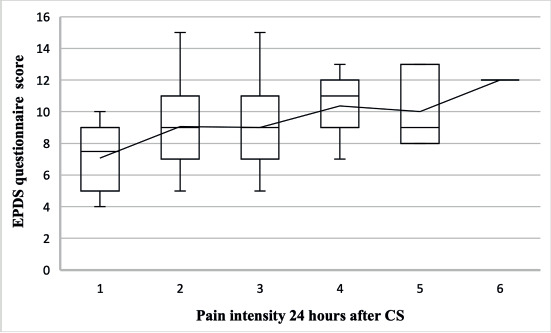
The relationships between the level of pain in the following hours after surgery and the risk of postpartum depression were significant for the entire group of subjects. Correlations were moderate (for measurement after 7 hours) and low (after 12 and 24 hours), but nevertheless showed that patients declaring higher levels of pain scored higher on the postpartum depression risk survey. Within-group correlations were only significant for the measurement after 7 hours in both groups and for the measurement after 6 hours in group A.
In addition, the relationship between the number of CS and the EPDS score was analyzed. None of the groups showed statistical significance in this respect. There was a weak negative correlation between the number of CS and the risk of postpartum depression. Detailed relationships are shown in Table 6.
Discussion
Pain after CS
Among women after CS, 79% experience pain in the surgical wound area up to two months after delivery, and in 18% the pain persists for up to six months. One in six patients develop chronic pain syndrome from acute postoperative pain [21]. Pain promotes postoperative complications, interferes with healing and regeneration processes, and impedes mobility and care of the newborn. Therefore, its effective and safe alleviation, which will enable full care and bonding between mother and child, is crucial not only for the well-being of the patient but also for the proper development of the newborn [22].
In clinical practice, the VAS and NRS scales are commonly used to assess pain. However, it should not be forgotten that the sensation of pain is modified by a number of factors, not solely due to the actual tissue damage. It appears that negative suggestion can modulate the anterior cingulate cortex, which connects the limbic system with the sensory cortex. A number of studies have shown that the very way of asking questions to the patient, by evoking negative emotions, can significantly affect the level of pain the patient declares [23]. In a study by Chooi et al. [23] it was shown that the way in which puerperae communicate, significantly influences their perception of postoperative feelings. The authors concluded that asking questions that shift patients’ attention to the comfort aspect makes them see their complaints as part of the healing and recovery process rather than as suffering [23]. In our study, reference was made to the above studies and in formulating the questions we started with the level of comfort, not pain.
Similar conclusions were drawn by Miu et al. [24] from a study on a group of patients following not only obstetric surgery, but also general and orthopedic surgery, among others. The authors highlight the effects of negative suggestion, in the form of adverse experience – the so-called nocebo effect. According to the authors, the small number of publications on this topic, confirms the lack of awareness among clinicians on the effects of negative communication [24].
In the present study, both patient comfort and pain questions were used to confirm whether there was a correlation between the two. The correlation was negative – as pain decreased 7 hours after CS, the comfort level of the patients increased significantly. It is therefore worth considering whether vocabulary with negative connotations should be used in midwifery practice. A better choice may be for medical staff to use open-ended questions, asking how they feel, or whether the patient needs something to make her more comfortable.
Mood disorders
The problem of postpartum mood disorders is underestimated and the topic is still downplayed. Polish authors point out the lack of awareness of this issue in the puerperae themselves, but also in the medical staff, which is a significant problem in our healthcare system [3,10,25]. Moreover, the COVID-19 pandemic, as shown in a recent study, additionally caused an increase in anxiety levels, incidence of mood disorders, and symptoms of PPD in a group of pregnant women [26]. Not being able to be visited by loved ones during hospitalization, feelings of isolation and fear of becoming ill are all factors that can negatively affect the wellbeing of puerperae. The problem may be exacerbated by a sense of inadequate care from hospital staff, as well as the presence of lactation problems [27].
In the present study, through the use of the EPDS questionnaire, the prevalence of increased risk of PPD was examined and to what extent it correlates with pain levels in puerperae. It should be emphasized that the EPDS is a screening tool that is not intended to and cannot replace a diagnosis by a psychiatrist. However, its estimated sensitivity in detecting depression is 80% [18]. At the hospitalization stage, the percentage of women with a high risk of PPD (score above 11 points) was 11.9% in total, of which the respondents were informed and advised to consult a psychologist. None of the women answered affirmatively to the question on suicidal thoughts.
Jaeshke et al. [28] estimated the prevalence of PPD in the population of puerperae in the Małopolskie Voivodeship at 15.2%, a percentage almost 30% higher than in our study. Moreover, in our study, the cut- off point for high risk of depression was 12, and in the study of Jaeshke et al., it was 13. The authors did not provide a full distribution of the results, but it is reasonable to suspect that if they had used 12 as the cut-off point, the percentage of puerperae diagnosed with PPD would have been even higher. The reason may be that the authors of the study also included puerperae after long, heavy natural deliveries, which is an additional risk factor for depression [28].
Similar results to Jaeshke et al. [28] were obtained by Ilska et al. [10] calculating the incidence of PPD to be 20%. The authors included women after emergency CS in the study, among others, and in this group of puerperae the risk of mood disorders is the highest [10]. Only women following elective surgery took part in our study.
Similarly, in the study by Fahrat et al. [29], in which the risk of PPD was found in every fourth woman after childbirth. However, studies have been conducted in mothers of children who have been in the intensive care unit after birth, which is an additional risk factor [29]. Mothers of newborns with a minimum Apgar score of 8 were eligible for our study.
In the Polish version of the questionnaire, the suggested cut-off point is a value of 12 or 13 [20]. For our study, a value of 12 was used, but some authors suggest that the risk of PPD, is already indicated by a value of 9 points. This value was adopted in their research by, among others, Teissedre and Chabrol [30], showing depression in 30% of puerperae. The mean EDPS questionnaire score for all subjects was 6.4 [30]. In our study, values greater than or equal to 9 were found in 58.3% of the subjects. This is significantly higher than in Teissedre and Chabrol’s study; however, the authors included women after both VB and CS in their assessment, with puerperae after CS accounting for only 17.3% of the study participants [30]. This is an important difference because, as research by Ilska et al. [10] showed, delivery by CS is an important risk factor for PPD. The authors highlighted the need for special care for female patients after CS, in the context of prevention of mood disorders and depression [10].
In our study, the mean score in the early puerperium was higher than in the repeat study performed after 4-6 weeks. The mean scores from both measurements were 8.75 and 7.79 respectively. This is in contrast to observations by other authors indicating that PPD increases in the following weeks of the puerperium [25]. It should be noted, however, that in our study, of the 49 women showing an increased risk of PPD at the hospitalization stage, only 11 women completed the questionnaire again, which fundamentally affects the results obtained. In the group of 29 subjects who completed the questionnaire twice, the average score increased from 8.14 to 8.24, confirming trends shown in other studies.
The aim of the present study, was to test the relationship between the level of pain after CS and the incidence of PPD risk. The significance of the correlation of pain levels at 7, 12 and 24 hours after CS with the EPDS results gives reason to conclude that effective pain relief, is a factor that reduces the risk of PPD. These findings are consistent with the observations of other authors. As stated by Lim et al. [18], each more point in the pain score increases the result obtained from the EDPS questionnaire by 8.3%. Ilska et al. [10] showed a positive correlation between pain levels and the occurrence of PPD symptoms. It has also been suggested that pain experienced already during or immediately after childbirth increases the risk of mood disorders [31]. Furthermore, both acute and subacute pain can increase vulnerability to mood disorders also in the chronic period – several months [18].
The relationship between the number of deliveries by CS and the incidence of PPD seems to be an interesting issue. The present study showed no significance in this respect, but only a very weak association in the form of a reduction in PPD risk with subsequent births. In this respect, the results of other studies are inconclusive. Febrianti et al. [32] considering puerperae after both CS and VB, also showed a decrease in PPD risk with subsequent deliveries. This may be explained by a greater awareness and better preparation of women going into subsequent pregnancies, in terms of the challenges of the perinatal period and the care of the newborn. However, having more children, while caring for their older siblings, can result in insufficient sleep and rest and consequently result in chronic fatigue, which is a risk factor for PPD [33].
The present study attempted to assess the effect of postpartum pain behind the occurrence of PPD in the immediate and late puerperium. An important limitation of the study was that it was carried out in a single center, on a relatively small group of puerperae. In addition, low responsiveness in the repeat EPDS survey, prevented reliable conclusions about mood disorders in the late postpartum period.
In addition, other factors that may influence stress levels and mood disorders were not included in the assessment, such as, for example, the socioeconomic situation of the respondents, or postpartum sleep difficulties or lactation problems. The results obtained should be seen as demonstrating a trend, the confirmation of which requires further research, on a larger group of subjects.
Research by other authors indicates that adverse and often even traumatic birth experiences not only significantly reduce women’s quality of life, but can also hinder bonding with the newborn, which in turn negatively affects its development. They also determine women’s reluctance to have further pregnancies. Therefore, the issue of perinatal pain relief is extremely important, not only from an individual perspective, but also from a societal perspective.
Conclusions
In this study, it was shown that higher levels of pain negatively affect the comfort of puerperae and are also associated with a higher risk of PPD. Although the standards of perinatal care in Poland have been modified several times in recent years, little attention is still paid to the care of women after CS, especially in terms of non-pharmacological methods of alleviating pain and the emotional state of puerperae. With an ever-increasing rate of surgical deliveries and, at the same time, an increasing number of women with mood disorders, it seems that the care of this group of patients needs more attention.
Disclosures and acknowledgements
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
This research received no specific grant from any funding agency in the public, commercial, or not-for- profit sectors.
Written consent was obtained from all the participants. The study was conducted in accordance with all the relevant national legislation, institutional policies and the principles of the Declaration of Helsinki. A favorable opinion from the Bioethics Committee of the Jagiellonian University was obtained for the study (opinion no. 1072.6120.137.2019).
Artificial intelligence (AI) was not used in the creation of the manuscript.